

When I ask patients who come in with chronic dermatitis what medications they have tried, many mention Nizoral and ketoconazole ointment. Strictly speaking, it is “ketoconazole cream,” but since many people call it “ketoconazole ointment,” I have used that term here for convenience as well.
It is true that Nizoral and ketoconazole ointment can help with seborrheic dermatitis, but some people still use these two products even when better options are available.
So, even among fungal infections, I have organized when these two products work well and when other products are a better choice.

목차
Three Types of Fungi That Cause Skin Problems
In the clinic, the fungi we see broadly fall into three types. Each has different food sources and habitats, and different susceptibility to antifungals.1
Fungi are classified by how they grow: filamentous dermatophytes that grow like threads, and single-celled, round-growing yeasts. The dermatophytes that cause athlete’s foot belong to the filamentous group, while Malassezia and Candida belong to the yeast group.
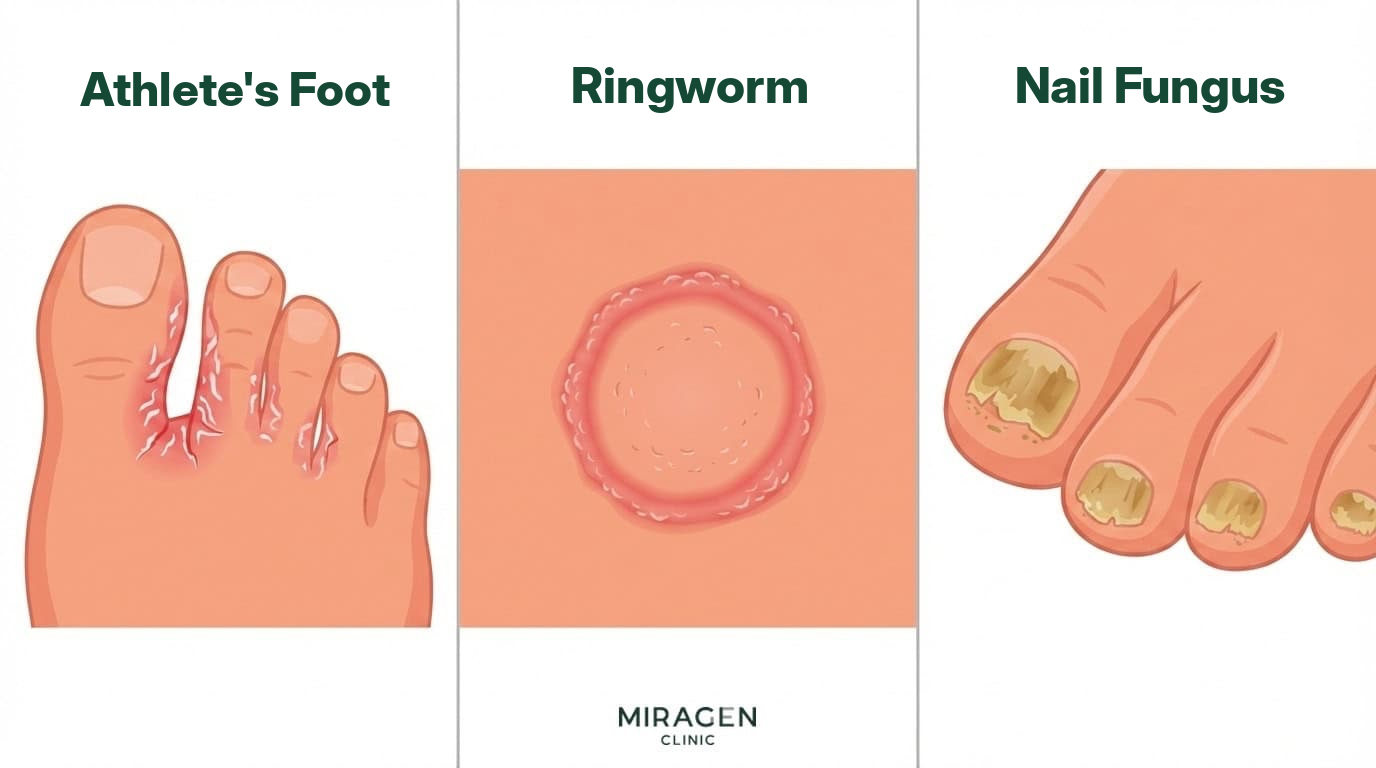
Dermatophytes
These are fungi that use keratin as a nutrient source. They invade keratin-rich tissues such as the stratum corneum, nails, and hair, and athlete’s foot, tinea corporis, tinea cruris, tinea capitis, and onychomycosis are all dermatophyte infections. They are also the most common type of superficial fungal infection worldwide.
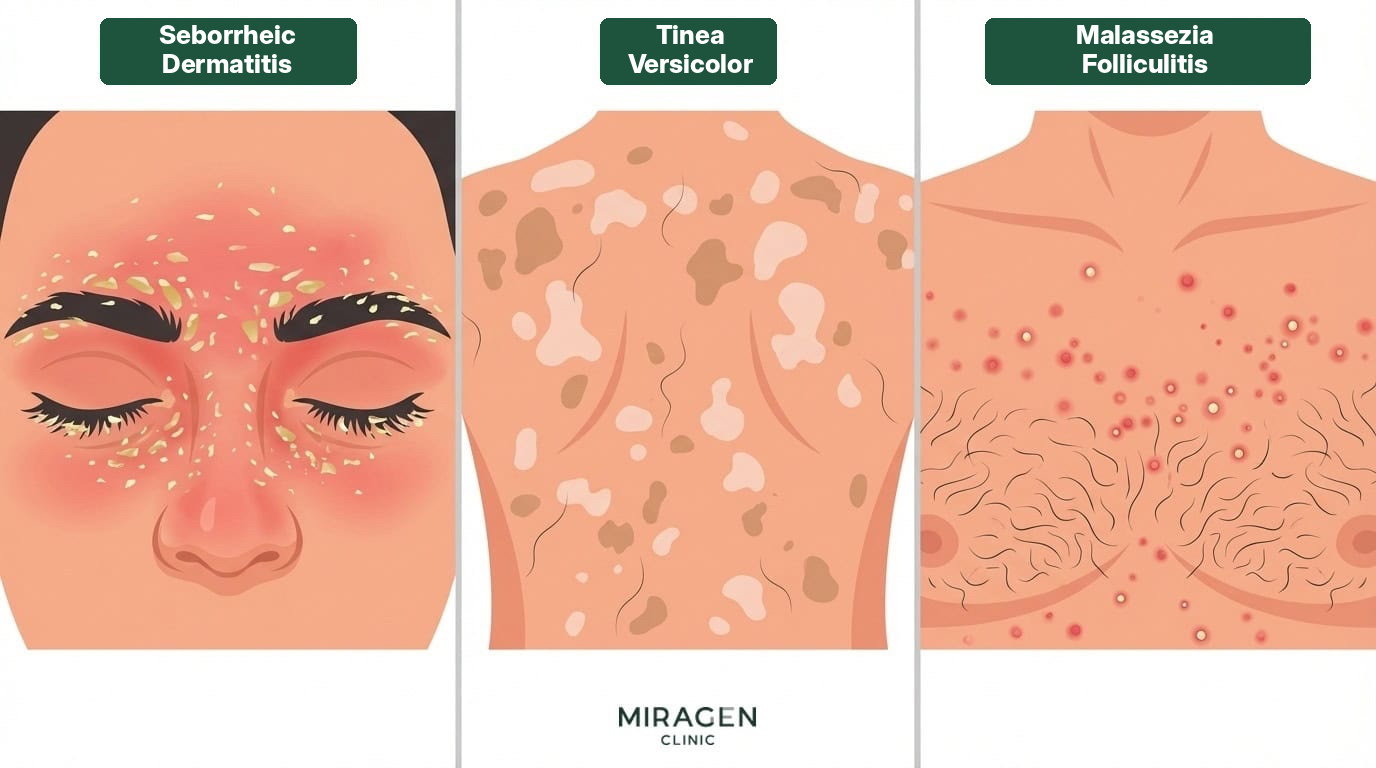
Malassezia
This is a yeast that feeds on sebum. It is present on normal skin, but when it overgrows, it causes seborrheic dermatitis or tinea versicolor. It mainly affects areas with high sebum production, such as the scalp, the facial T-zone, the chest, and the back.
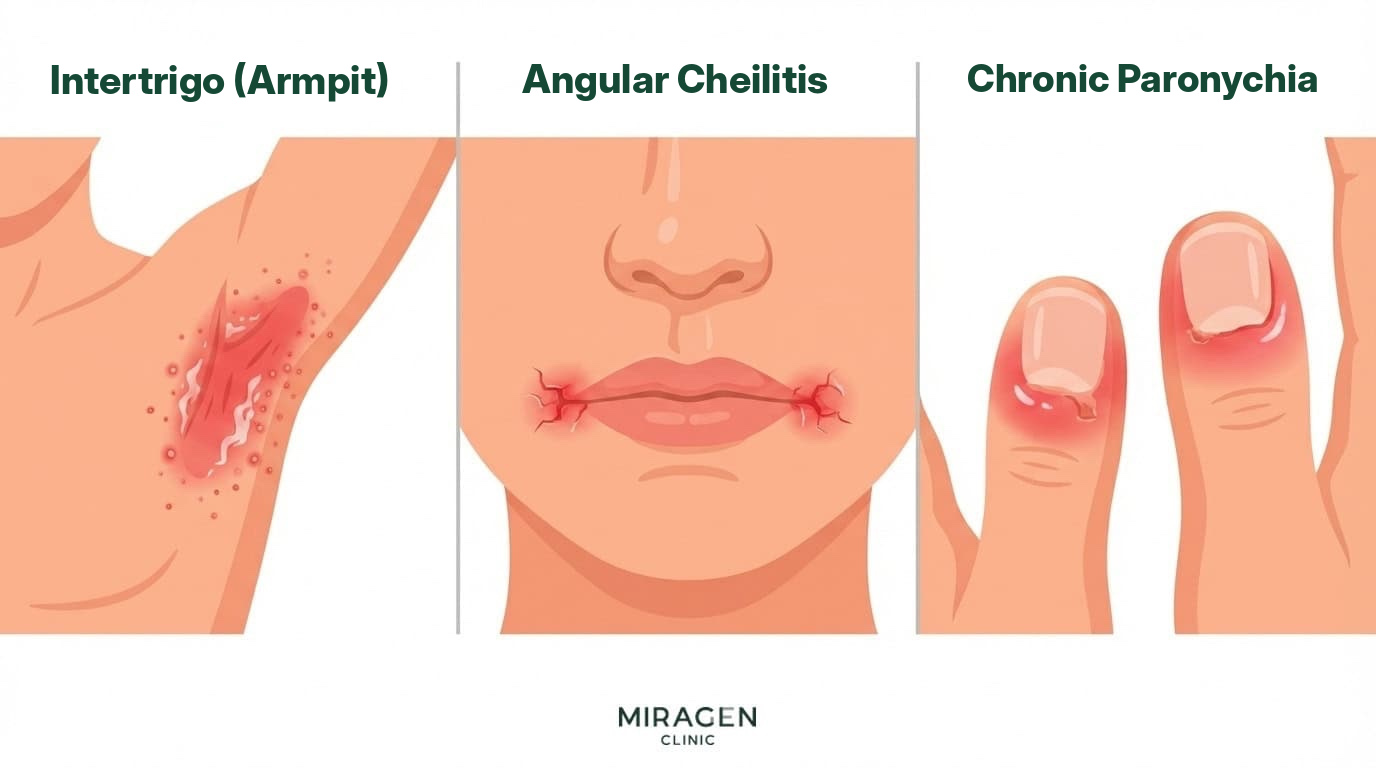
Candida
This is a yeast that proliferates in warm, humid environments. It causes cutaneous candidiasis in skin folds such as the armpits, groin, and under the breasts,2 and is more common in infants wearing diapers and in people with weakened immunity.
How Antifungals Kill Fungi
The main target of antifungals is ergosterol, a key component of the fungal cell membrane. Each drug class attacks ergosterol differently, so the range of fungi it is effective against also differs.1
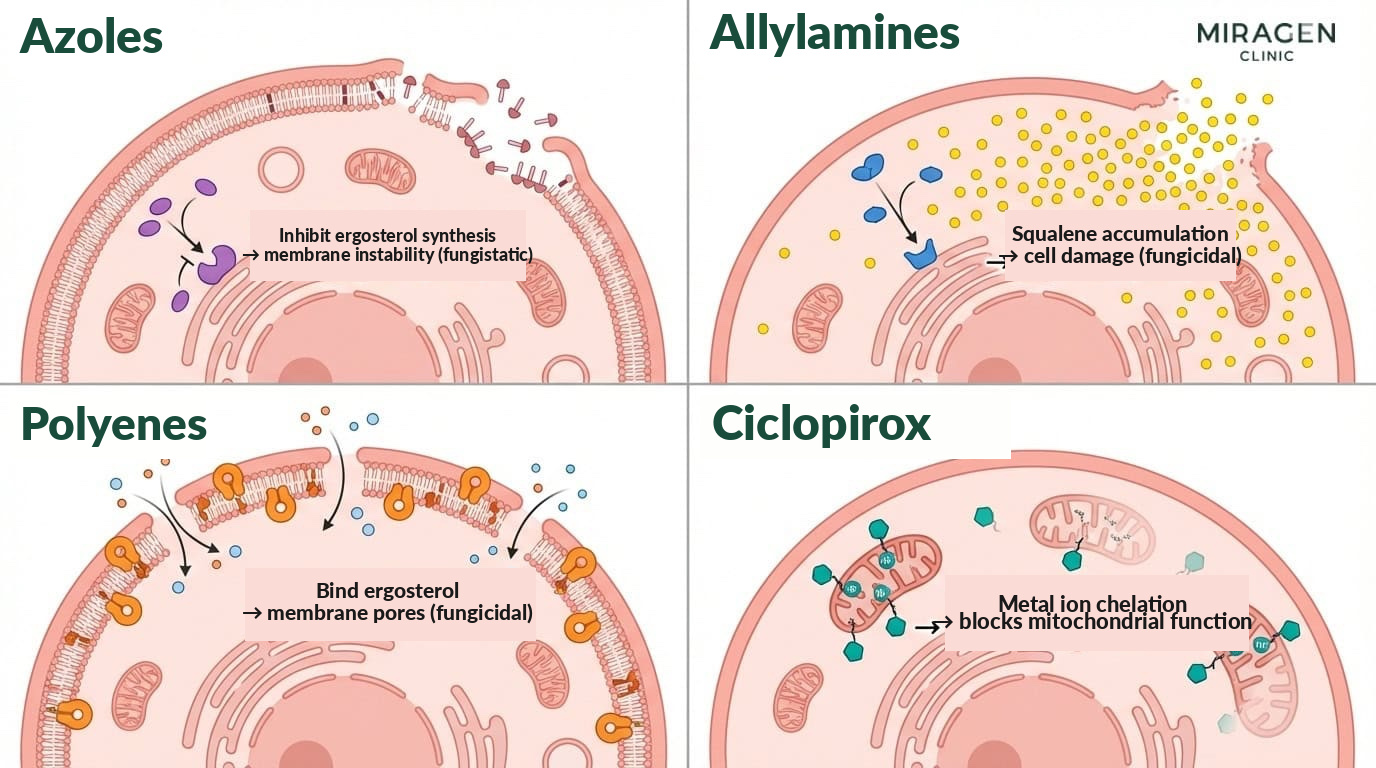
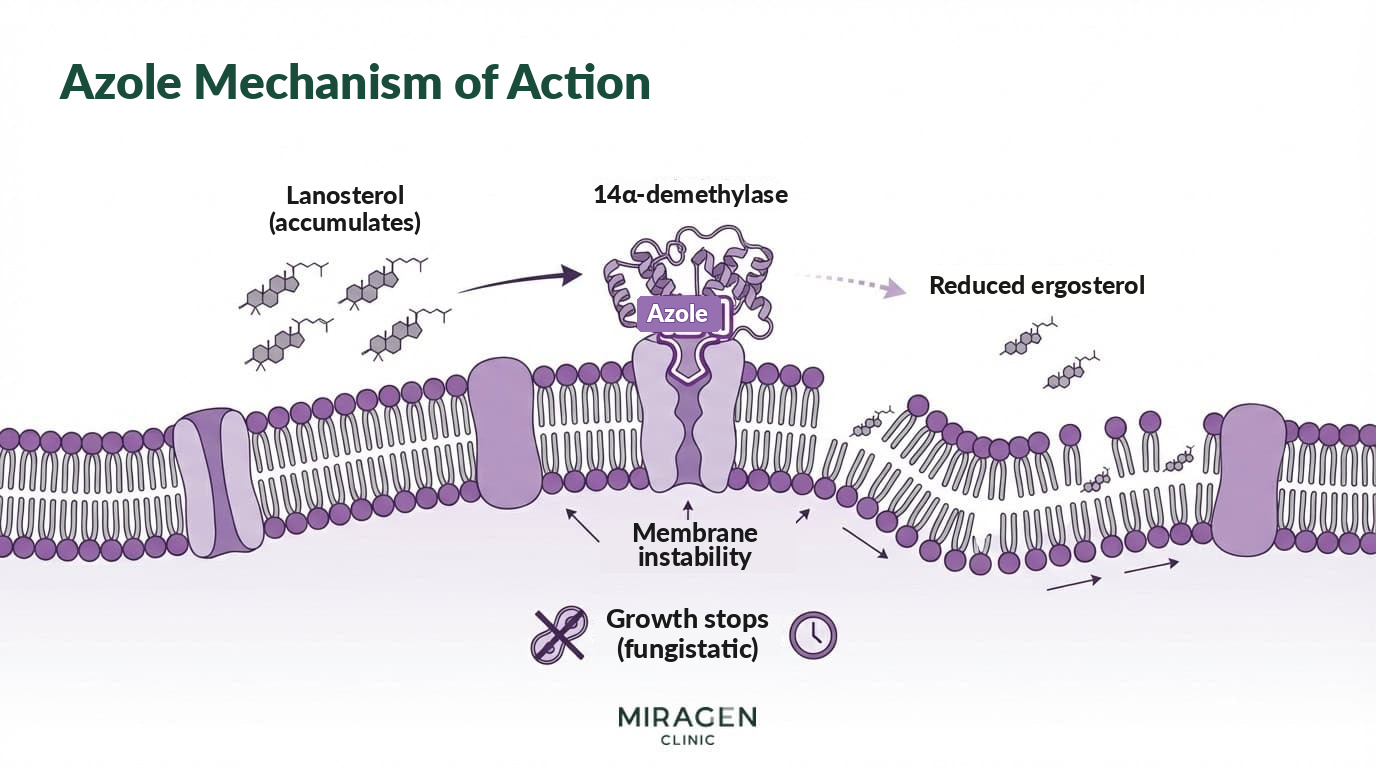
Azoles
They inhibit lanosterol 14α-demethylase, reducing ergosterol synthesis. As the cell membrane becomes unstable, fungal growth stops, but the fungus is not killed directly—these are fungistatic agents. Complete clearance is left to the immune system.
Because they have a broad spectrum, they are effective against all three: dermatophytes, Malassezia, and Candida. In particular, they have the strongest evidence for Malassezia.3
Representative products include Nizoral solution (ketoconazole), ketoconazole ointment (ketoconazole), Jublia topical solution (efinaconazole), and Canesten cream (clotrimazole). All four are topical agents.
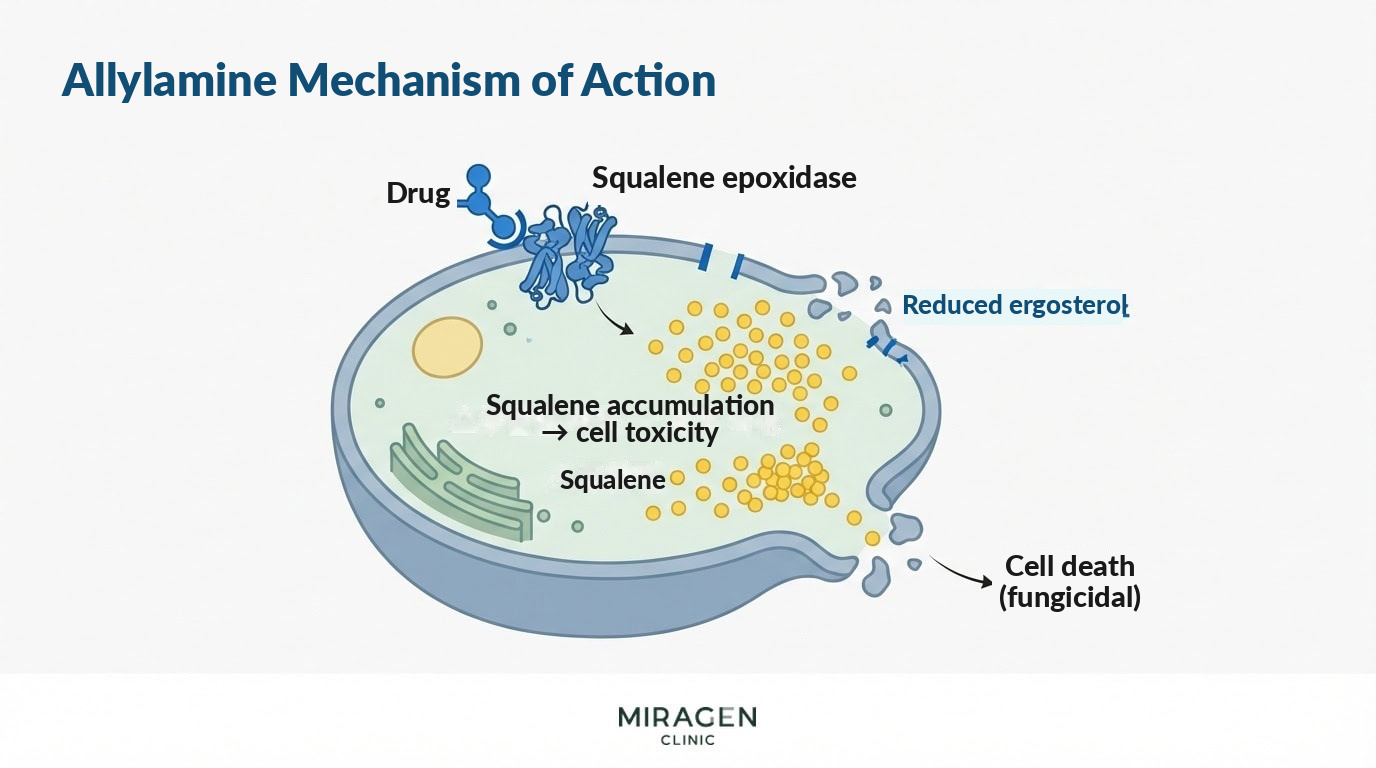
Allylamines
Like azoles, they block ergosterol synthesis, but they inhibit squalene epoxidase, which is an earlier step than the enzyme targeted by azoles. As a result, unused squalene accumulates in the cell, and this itself is toxic to fungal cells.
Because ergosterol reduction and squalene toxicity act together, allylamines are fungicidal agents that directly kill fungi. In an analysis combining multiple clinical trials, the cure rate of allylamines was 70%, higher than 47% for azoles.4 Thanks to their fungicidal action, treatment tends to be shorter and recurrence rates tend to be lower.
However, allylamines are drugs specialized for dermatophytes. Their effect against Malassezia or Candida is limited, so azoles are more suitable for yeast infections.5
Representative products include the topical Lamisil cream (terbinafine) and the oral Lamisil tablet (terbinafine).
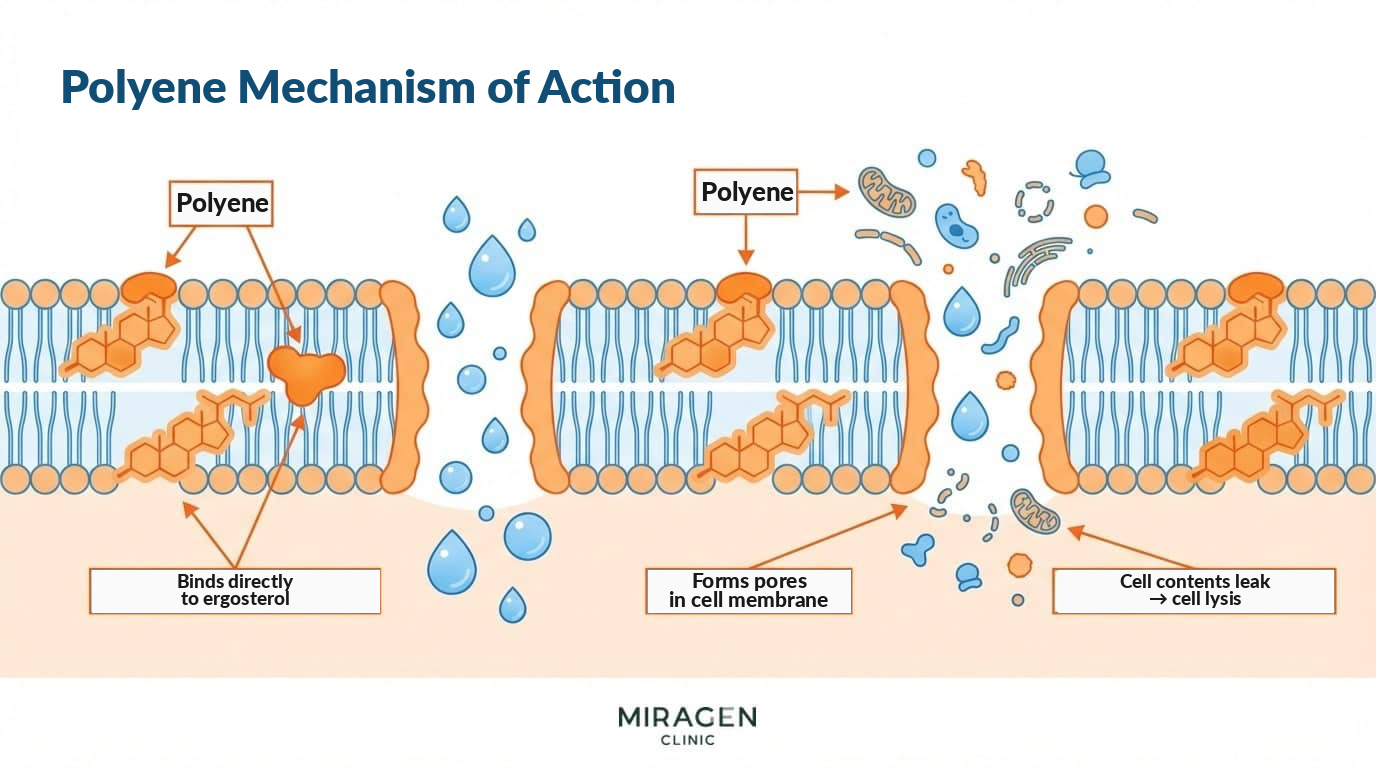
Polyenes
They do not interfere with synthesis; instead, they bind directly to ergosterol that has already been made. This creates physical holes in the cell membrane, causing contents to leak out and the fungus to lyse.1 They work well for Candida but not for dermatophytes, so they are mainly used for cutaneous candidiasis.
A representative product is Mycostatin ointment (nystatin).
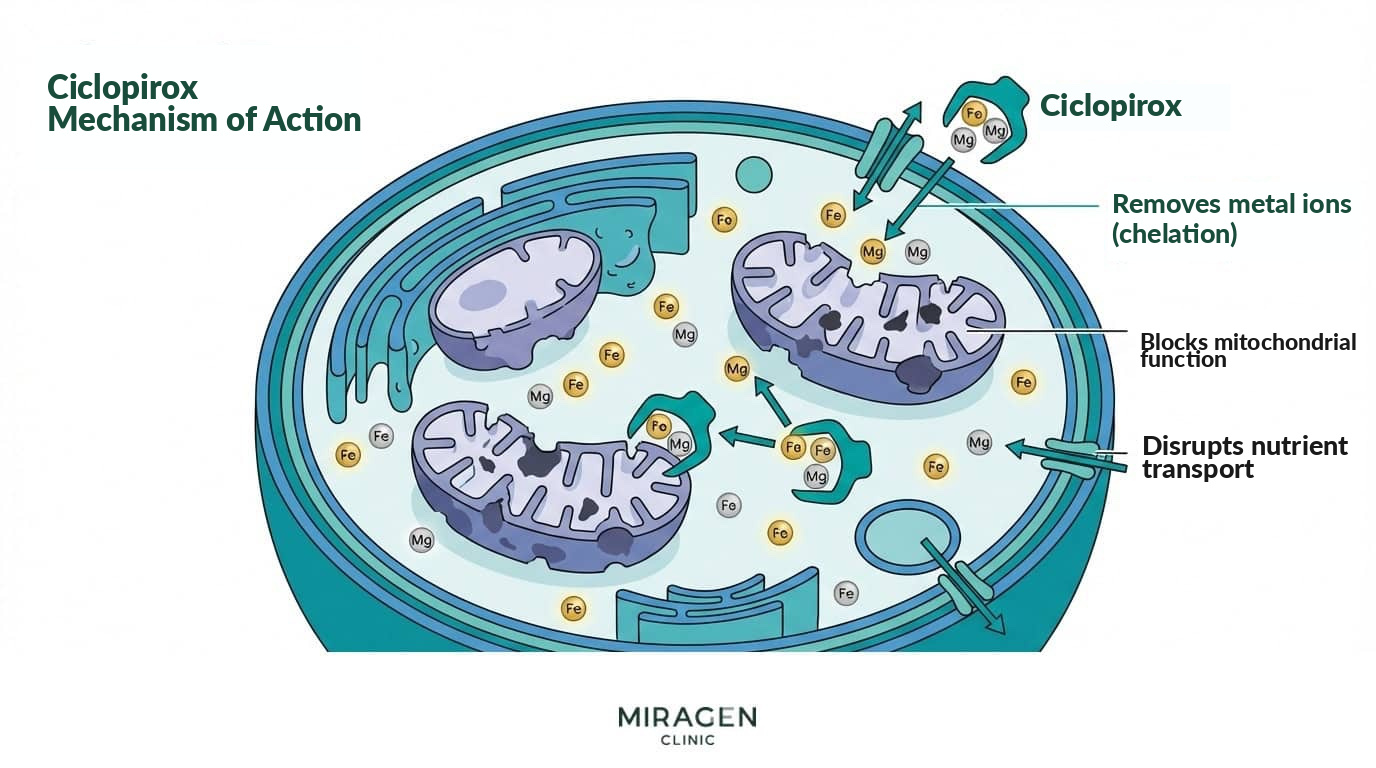
Ciclopirox
Its mechanism differs from the three classes above. It chelates metal ions such as iron, disrupting fungal mitochondrial function and nutrient transport. Because it bypasses the ergosterol pathway, it is the broadest-spectrum antifungal. It covers dermatophytes, Candida, and Malassezia, and there are reports that it is effective even against azole-resistant Candida species.6
A representative product is Loprox gel (ciclopirox).
Which Antifungal to Use for Which Fungus
Dermatophytes (Athlete’s Foot, Tinea Corporis, Tinea Cruris) | Allylamines
For dermatophyte infections, the first-line option is a topical terbinafine (an allylamine), such as Lamisil cream. Thanks to its fungicidal action, it has a higher cure rate and tends to have fewer recurrences than azoles.4,5 The standard regimen is application 1–2 times daily for 2–4 weeks. Even after symptoms resolve, continuing for an additional 1–2 weeks helps eliminate remaining fungi.1
If the affected area is extensive or does not respond to topical treatment, oral terbinafine (Lamisil tablet) 250 mg is taken for 1–2 weeks. For onychomycosis as well, oral therapy has the highest cure rate, but if liver function is poor or drug interactions are a concern, applying Jublia (efinaconazole 10% topical solution) is also an option. Because it penetrates the nail well, cure rates have improved meaningfully compared with older topical agents. Dermatophytes with reduced response to terbinafine have been reported in some regions recently, but they are still uncommon in Korea.7
Malassezia (Seborrheic Dermatitis, Tinea Versicolor) | Azoles
For Malassezia-related conditions, topical ketoconazole (an azole)—such as Nizoral and ketoconazole cream—has the strongest evidence. In an analysis combining multiple clinical trials (12 studies, 3,253 participants), it showed a 31% higher improvement rate than placebo, meaning that treating five people leads to one person showing clear improvement.3 Ciclopirox (Loprox gel) shows a similar level of efficacy.3 Nizoral is the most commonly used topical ketoconazole product in Korea.
Candida | Azoles, Polyenes
For Candida infections, apply a topical clotrimazole (an azole), such as Canesten cream, or a topical nystatin (a polyene), such as Mycostatin ointment, for 2 weeks.2 Since improving the moist environment itself is key to preventing recurrence, keeping the area dry and wearing breathable clothing is as important as medication.
This is a summary table of the representative products by active ingredient discussed above.
| Product Name | Main Indications | Category | Over-the-Counter | Active Ingredient | Class |
|---|---|---|---|---|---|
| Nizoral | Seborrheic Dermatitis, Tinea Versicolor, Dandruff | Topical | Available | Ketoconazole | Azoles |
| Canesten Cream | Athlete’s Foot, Candida | Topical | Available | Clotrimazole | Azoles |
| Lamisil Cream | Athlete’s Foot, Tinea | Topical | Available | Terbinafine | Allylamines |
| Loprox Gel | Interdigital Tinea Pedis, Seborrheic Dermatitis | Topical | Available | Ciclopirox | Ciclopirox |
| Mycostatin | Cutaneous Candidiasis | Topical | Available | Nystatin | Polyenes |
| Jublia | Onychomycosis | Topical | Prescription Required | Efinaconazole | Azoles |
| Lamisil Tablet | Onychomycosis, Extensive Tinea | Oral | Prescription Required | Terbinafine | Allylamines |
| Sporanox | Onychomycosis, Tinea Corporis | Oral | Prescription Required | Itraconazole | Azoles |
| Diflucan | Candidiasis, Tinea Versicolor | Oral | Prescription Required | Fluconazole | Azoles |
Each antifungal works best against different fungi. Therefore, confirming the causative fungus and choosing an antifungal accordingly is the first step in treatment.
References
- Hay R. Therapy of Skin, Hair and Nail Fungal Infections. J Fungi (Basel). 2018;4(3):99.
- Müller VL, Kreuter A, Uhrlaß S. Relevant aspects of Candida species in dermatology: An overview. Dermatologie (Heidelb). 2025;76(9):544-550.
- Okokon EO, Verbeek JH, Ruotsalainen JH, et al. Topical antifungals for seborrhoeic dermatitis. Cochrane Database Syst Rev. 2015;(5):CD008138.
- Crawford F, Hollis S. Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst Rev. 2007;(3):CD001434.
- Gupta AK, Foley KA, Versteeg SG. New Antifungal Agents and New Formulations Against Dermatophytes. Mycopathologia. 2017;182(1-2):127-141.
- Sonthalia S, Agrawal M, Sehgal VN. Topical Ciclopirox Olamine 1%: Revisiting a Unique Antifungal. Indian Dermatol Online J. 2019;10(4):481-485.
- Gupta AK, Wang T, Piguet V. Recalcitrant dermatophytosis: clinicomycological features and challenges in management. Expert Opin Pharmacother. 2025;26(18):1985-1996.
Frequently Asked Questions
Can I use athlete’s foot medication for seborrheic dermatitis?
Terbinafine, a key ingredient in athlete’s foot medications, is a fungicidal agent specialized for dermatophytes. Its effect against Malassezia, the cause of seborrheic dermatitis, is limited, so it is better to choose an ingredient that is effective against Malassezia, such as ketoconazole or ciclopirox.
How long should I apply an antifungal ointment?
In general, athlete’s foot or tinea is treated for 2–4 weeks, tinea versicolor for 2–3 weeks, and cutaneous candidiasis for 2 weeks. Even if symptoms disappear, completing the prescribed duration helps reduce recurrence.
Can antifungals also develop resistance?
Dermatophytes that do not respond to terbinafine have been reported in some regions recently. They are still uncommon in Korea, but using antifungals at an appropriate dose and for an appropriate duration is the foundation of preventing resistance.

We treat atopic dermatitis, rosacea, and seborrheic dermatitis.
Thanks to the valuable reviews you have shared in the community, many of you visit us even from far away.
We will repay you with sincere, attentive care.
DK Han
Chief Director, MIRAGEN Clinic
Graduate of University of Michigan, Ross School of Business
Graduate of Chungnam National University School of Medicine
(Former) Representative Director of Ewha Phoenix Rehabilitation Hospital
(Current) Representative Director of MIRAGEN Clinic