

When a red rash appears on the cheeks of a one- to two-month-old baby, what parents are usually most curious about is whether it is heat rash or newborn atopic dermatitis. They may look similar, but heat rash typically improves on its own within a few weeks, whereas newborn atopic dermatitis can lead to allergies that may persist for life if not treated early—so the approach is completely different.1
We have organized three key criteria for telling the two apart, and what to do after it is confirmed to be atopic dermatitis.
목차
How to Tell Heat Rash from Newborn Atopic Dermatitis
Heat rash is not a medical term. It is a catch-all term for skin troubles seen in newborns, including neonatal acne and seborrheic dermatitis. Among these, the key criteria for distinguishing newborn atopic dermatitis are whether itching is present and the condition of the diaper area.2
| Condition | Neonatal Acne | Seborrheic Dermatitis | Atopic Dermatitis |
|---|---|---|---|
| Main symptoms | Not itchy | Hardly itchy | Severe itching |
| Appearance | Tiny papules and pustules | Greasy yellow scales | Dryness, redness, oozing |
| Common areas | Face, upper chest | Scalp, diaper area | Face, outer arms and legs |
| Diaper area | No involvement | Common | Usually clear |
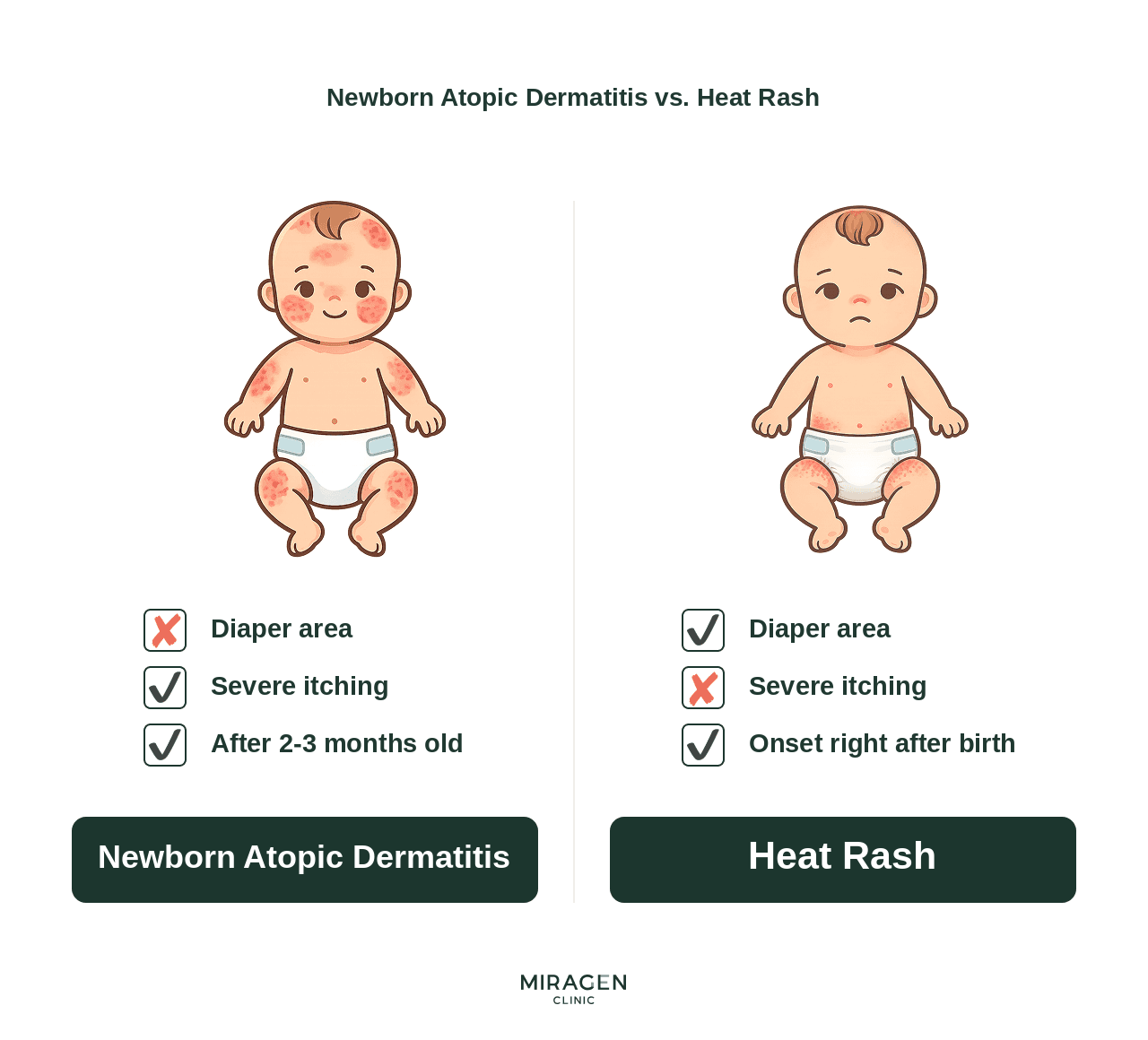
1. Itching
With neonatal acne or seborrheic dermatitis, babies are rarely itchy. In contrast, the most decisive symptom of newborn atopic dermatitis is severe itching.2 In atopic skin, the function of barrier proteins such as filaggrin is reduced, creating gaps in the skin barrier,3 and external irritants penetrate through these gaps, triggering immune reactions and itching at the same time.4
Because newborns cannot say “it itches,” you have to judge by their behavior. If your baby repeatedly rubs their face against a blanket or a parent’s clothes, keeps bringing their hands to their face, or becomes fussy at night and has disrupted sleep, you should suspect newborn atopic dermatitis rather than simple heat rash.
2. Condition of the diaper area
Newborn atopic dermatitis rarely appears in the diaper area.2 If the rash is severe on the scalp, face, and outer arms and legs but the diaper area is clear, atopic dermatitis is more likely.
There are several reasons the skin inside the diaper tends to stay clear. Humidity is higher inside the diaper, which reduces moisture loss from the skin, and urea in urine acts as a natural moisturizing factor. The diaper also physically prevents scratching, helping break the itch–scratch cycle.5 If you compare the skin to a brick wall, the inside of the diaper has enough “cement” (moisture), leaving fewer gaps for external irritants to get in.
Seborrheic dermatitis, on the other hand, commonly occurs in the diaper area. Therefore, the condition of the diaper area is a very useful clue for distinguishing the two conditions.
3. Timing of onset
Heat rash (neonatal acne · seborrheic dermatitis) usually appears at 2–4 weeks of age and improves on its own within a few weeks. In contrast, newborn atopic dermatitis typically begins in earnest after 2–3 months of age. In one birth cohort study, the median age of atopic dermatitis onset in full-term infants was 4 months.6
Even if the rash appears before 2 months of age, if itching is clear and the diaper area is clean, I keep the possibility of atopic dermatitis in mind and monitor the course. This is because itching and distribution are more decisive diagnostic criteria than timing.
What to Do After Confirming Newborn Atopic Dermatitis
If newborn atopic dermatitis is suspected based on the criteria above, you can start the following three steps right away.
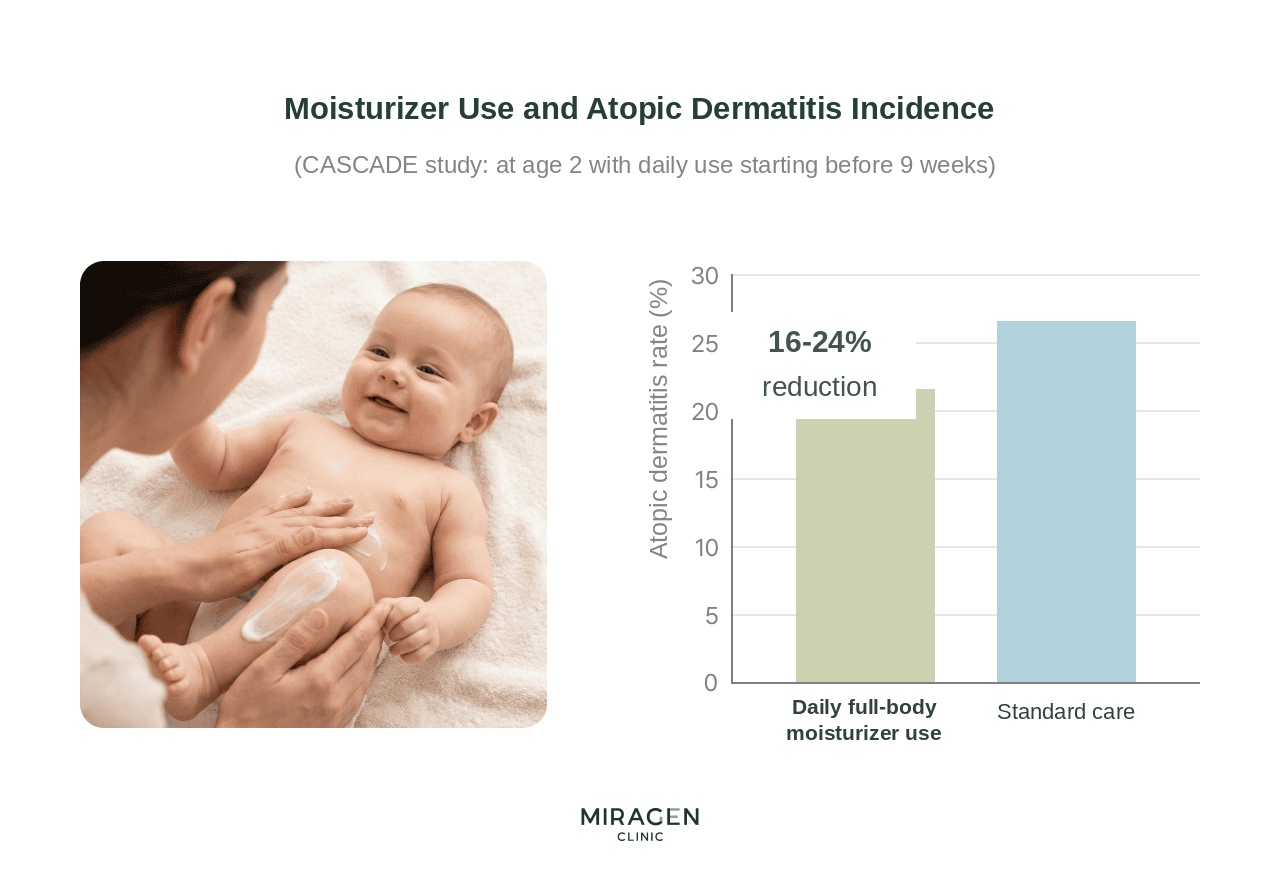
Moisturizer care
The first step in managing newborn atopic dermatitis is moisturizing. In a meta-analysis in which emollients were applied early and consistently in high-risk infants, the risk of developing atopic dermatitis decreased by about 36%.7 The rule is to apply a generous amount within 3 minutes after bathing while the skin is still moist, at least twice a day.
When choosing an emollient, I recommend a cream rather than a lotion. Creams work better as a protective barrier, and they typically contain fewer preservatives than more water-based lotions, making irritation less likely. For how to choose an emollient when atopic dermatitis is suspected, please refer to the MD Cream Guide.
Environmental management
Maintain an indoor temperature of 20–22°C and humidity of 50–60%. In winter, when heating is strong, indoor air can easily become dry, so using a humidifier is recommended. Use 100% cotton for clothing and bedding that touches the skin directly, and choose fragrance-free detergent for laundry. Avoid fabric softener whenever possible, as residual chemicals can irritate the skin.
Signs you should see a doctor
If symptoms do not improve with moisturizing and environmental management alone, or if you notice any of the signs below, medical evaluation is needed.
- Repeatedly losing sleep at night due to itching
- Cracked skin or oozing
- A rash that spreads quickly from the face to the arms, legs, and trunk
- Fever with a rapid worsening of the skin condition
During evaluation, we determine whether it is atopic dermatitis by comprehensively assessing the distribution of symptoms, the degree of itching, family history, and more. If needed, medication may be started in addition to emollients. Because infantile atopic dermatitis can be the starting point of the atopic march that progresses to food allergy, rhinitis, and asthma,8 early management is especially important. If you would like to learn about the overall causes of atopic dermatitis and the direction of treatment, please refer to the Atopic Dermatitis Guide.
References
- Frei R, Depner M, Karvonen AM, et al. Phenotypes of Atopic Dermatitis Depending on the Timing of Onset and Progression in Childhood. JAMA Pediatr. 2017;171(7):655-662.
- Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338-351.
- Palmer CN, Irvine AD, Terron-Kwiatkowski A, et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet. 2006;38(4):441-446.
- Jeskey J, et al. Atopic Dermatitis: A Review of Diagnosis and Treatment. J Pediatr Pharmacol Ther. 2024;29(6):587-597.
- Jazdarehee A, et al. Potential Mechanisms of the Sparing of Atopic Dermatitis in the Diaper Region: A Scoping Review. J Cutan Med Surg. 2022;26(4):398-407.
- Gerner T, et al. Differences in Occurrence, Risk Factors and Severity of Early-onset Atopic Dermatitis among Preterm and Term Children. Acta Derm Venereol. 2022;102:adv00726.
- Liang J, et al. Systematic review and network meta-analysis of different types of emollient for the prevention of atopic dermatitis in infants. J Eur Acad Dermatol Venereol. 2023;37(3):501-510.
- Tsuge M, et al. Current Insights into Atopic March. Children (Basel). 2021;8(11):1067.
Frequently Asked Questions
If you leave heat rash alone, will it turn into atopic dermatitis?
Heat rash (neonatal acne · seborrheic dermatitis) does not “progress” into atopic dermatitis. They are separate conditions with different causes and mechanisms. Heat rash usually improves within a few weeks with environmental management alone (indoor temperature 20–22°C, humidity 50–60%). However, a rash you thought was heat rash may actually have been an early symptom of atopic dermatitis, so if itching is present or there is no rash in the diaper area, we recommend that you seek medical evaluation.
Can I use a steroid ointment for newborn atopic dermatitis?
Yes, if needed, it can be used with a doctor’s prescription. However, because newborns have a different body surface area-to-weight ratio than adults, systemic absorption is higher, so you must be prescribed an ointment of appropriate potency and use it only on the designated areas and for the prescribed duration. If you would like to learn about differences by potency class, please refer to the Steroid Ointment Potency Guide.
If my baby has atopic dermatitis, will they also develop food allergies or asthma?
Babies with atopic dermatitis have a weakened skin barrier, making sensitization to environmental antigens more likely. As a result, the “atopic march” may occur, progressing sequentially to food allergy, allergic rhinitis, and asthma. This is why actively restoring the skin barrier early is also important for preventing allergic diseases later on.

We treat atopic dermatitis, rosacea, and seborrheic dermatitis.
Thanks to the valuable reviews you have shared in the community, many of you visit us even from far away.
We will repay you with sincere, attentive care.
DK Han
Chief Director, MIRAGEN Clinic
Graduate of University of Michigan, Ross School of Business
Graduate of Chungnam National University School of Medicine
(Former) Representative Director of Ewha Phoenix Rehabilitation Hospital
(Current) Representative Director of MIRAGEN Clinic