

When I ask patients who come in for facial atopic dermatitis which ointments they have tried, I very often hear that they were too afraid to use steroid ointments, but have tried various non-steroidal ointments.
They mention a wide range of products—from OTC options like Bepanthen and Biafine, to prescription medications like Protopic and Elidel, and even overseas direct-purchase products like Rutinib, Opzelura, and Tofacitinib.
Because facial skin is thin, topical medications are absorbed more readily—so it is only natural to worry about steroid side effects.

As a physician, I cannot recommend unapproved products in Korea such as Rutinib or Tofacitinib as atopic dermatitis ointments, but I am writing this because I believe it would be helpful to provide accurate information to those who are already using them. Below, I will compare—based on evidence—the seven non-steroidal topical treatments most frequently mentioned by patients who visit for facial atopic dermatitis.
목차
Why is facial atopic dermatitis different?
Compared with the arms or legs, the stratum corneum of facial skin is much thinner. A thinner stratum corneum means topical medications are absorbed more, and more quickly, into the skin.1
That is why steroid ointments can be very effective—but side effects can also be more severe. Skin atrophy and telangiectasia are concerns, but the biggest issue is rebound. After using steroids for a long time and then stopping, symptoms such as worse-than-before redness and burning can occur. Studies analyzing these rebound cases show that most occurred on the face.2 This is why many people look for non-steroidal ointments when facial atopic dermatitis develops.
Ointment vs. cream | Which formulation is better?
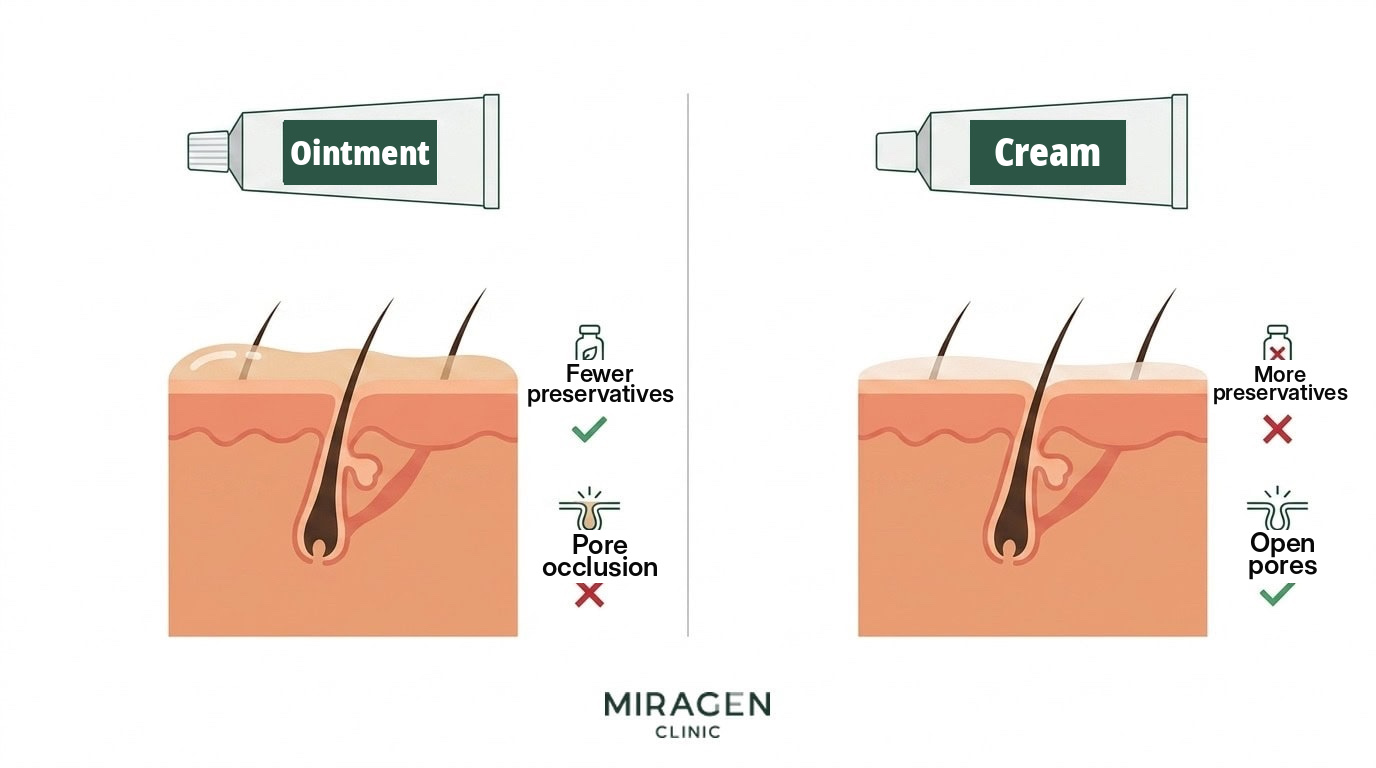
Even with the same active ingredient, ointments and creams use different bases. Ointments are oil-based and contain little to no water, while creams are emulsions that mix oil and water. This difference matters quite a bit for facial atopic dermatitis.
The advantage of ointments is safety. Because they contain little or no water, they require few preservatives to inhibit microbial growth. Creams, on the other hand, need preservatives because of their water content, and preservatives (such as benzyl alcohol, propylene glycol, and sorbic acid) have consistently been reported to cause contact dermatitis in patients with a compromised skin barrier.3
The downside of ointments is acne. The oils can clog pores. Because the face has a high density of pores, it is fairly common for new acne to develop or existing acne to worsen after applying an ointment. In fact, I sometimes see patients return because their acne worsened after being prescribed Protopic ointment. The feel is also an issue: it is not easy to keep applying a sticky, greasy ointment to the face consistently.
European expert consensus statements reflect this as well, recommending ointments for moderate-to-severe disease or for the body, and creams for the face or for mild disease.4
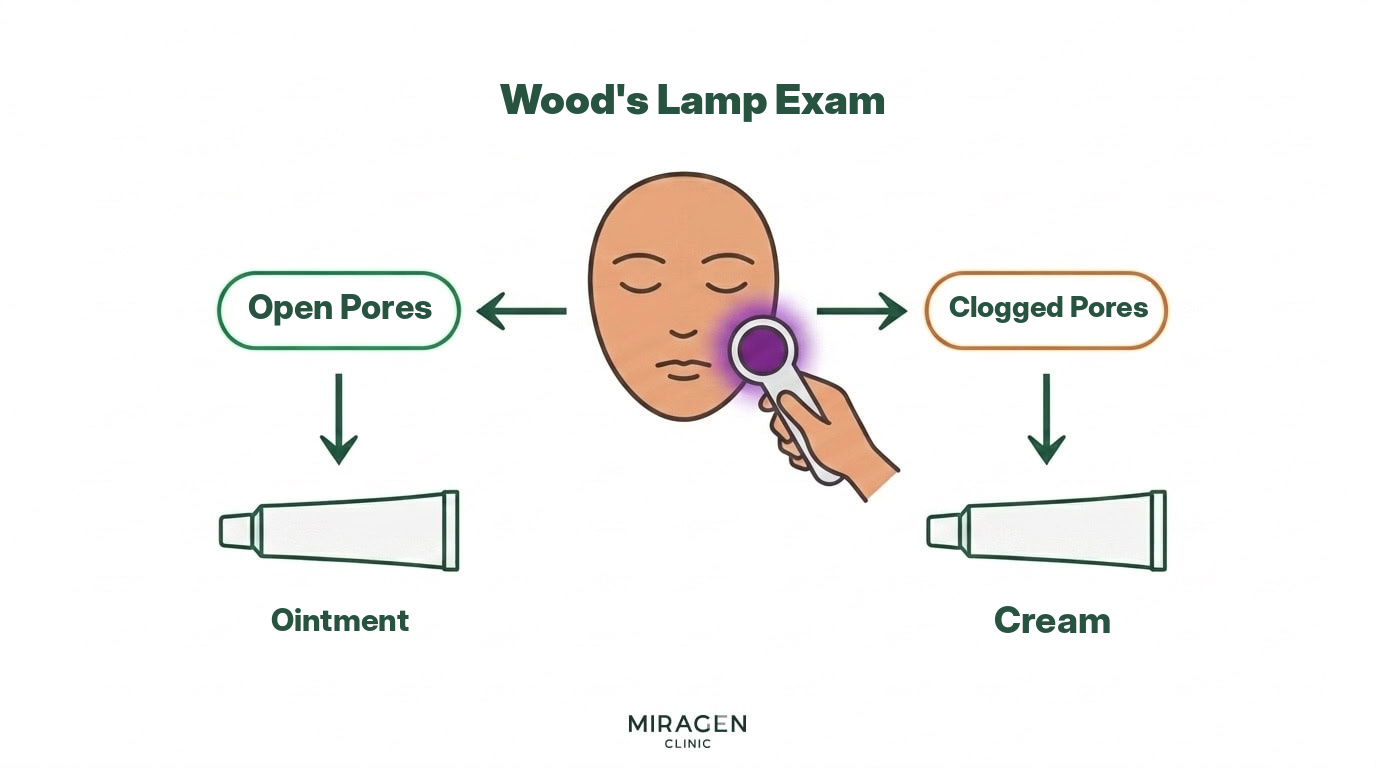
In summary, ointments are generally better for efficacy and safety, but if you have acne, using a cream is more practical. After checking for pore blockage with a Wood’s lamp exam, I prescribe a cream formulation for patients who seem likely to develop acne.
| Ointment | Cream | |
|---|---|---|
| Preservatives | None or minimal | Relatively more |
| Risk of contact dermatitis | Low | Relatively high |
| Pore occlusion/acne | May trigger | Relatively less |
| Texture/feel | Sticky | Lightweight |
| Suitability for the face | Preferred if no acne | Preferred if acne is present |
Comparing 7 non-steroidal atopic dermatitis ointments
The relative efficacy of non-steroidal atopic dermatitis ointments can be understood by synthesizing results from multiple clinical trials. A 2024 analysis by the Cochrane team (291 trials, 45,846 participants) already compared Protopic, Elidel, Anzupgo, and Opzelura, and the relative efficacy of Tofacitinib and Bepanthen can be indirectly compared using separate clinical trials.5
| Active ingredient | Representative product | Formulation | Efficacy rating | Approved in Korea |
|---|---|---|---|---|
| Tacrolimus 0.1% | Protopic 0.1% | Ointment | ★★★★ | O (covered) |
| Delgocitinib 0.5% | Anzupgo | Cream | ★★★★ | Chronic hand eczema only (non-covered) |
| Ruxolitinib 1.5% | Opzelura, Rutinib | Cream | ★★★★ | X (direct purchase) |
| Tacrolimus 0.03% | Protopic 0.03% | Ointment | ★★★ | O (covered) |
| Pimecrolimus 1% | Elidel | Cream | ★★ | O (covered) |
| Tofacitinib 2% | Tofatas | Ointment | ★★ | X (direct purchase) |
| Dexpanthenol 5% | Bepanthen, D-Panthenol | Ointment | ★ (adjunct) | OTC |
Protopic 0.1% | The most well-validated choice

Tacrolimus 0.1% ointment is the benchmark non-steroidal atopic dermatitis ointment, supported by more than 20 years of clinical evidence. In a Cochrane review analyzing six clinical trials (1,640 participants), 0.1% showed an 18% significantly higher physician-assessed improvement rate than 0.03%.6 In three head-to-head trials, it was clearly more effective than pimecrolimus cream with similar safety.7 The 2024 Cochrane analysis also ranked Protopic 0.1% as one of the most effective non-steroidal topical treatments.5
The downside is stinging and burning for the first 2–3 days. This occurs when TRPV1 receptors are stimulated and substance P and CGRP are released all at once. However, this process is not necessarily harmful. If repeated stimulation depletes substance P and CGRP stored in nerve endings, itching, stinging, and redness may decrease over the long term. The initial discomfort usually settles within a week, and applying it after refrigeration can reduce irritation. You can find more details in the separate posts on Protopic and on choosing the concentration for facial use.
Anzupgo, Opzelura, Ruti | New drugs comparable to Protopic


Anzupgo (delgocitinib) and Opzelura/Rutinib (ruxolitinib) are topical treatments from a new class called JAK inhibitors. In a pooled analysis of 291 clinical trials, these two drugs showed efficacy nearly comparable to Protopic 0.1%.5 In an analysis published in 2026, ruxolitinib was even rated as having the highest efficacy among non-steroidal topical treatments.8
In particular, significant improvement was confirmed in studies targeting facial/neck dermatitis. In a face/neck-specific clinical trial, ruxolitinib showed significant improvement in just two weeks,9 and delgocitinib improved both satisfaction and symptoms in patients who switched from existing steroids or tacrolimus.10
However, the real-world constraints are substantial. In Korea, Anzupgo is approved only for chronic hand eczema and is non-covered (the pharmacy acquisition cost for 60 g alone is KRW 690,000), and Opzelura/Rutinib are not approved at all, so they can only be obtained via overseas direct purchase. Their efficacy is Protopic-level and the cream formulation may feel better, but in terms of cost and accessibility, it is difficult for them to be a first-line choice.
Elidel, Tofacitinib | One step down


Pimecrolimus 1% cream (Elidel) has a lower anti-inflammatory effect than Protopic. In head-to-head clinical trials, it consistently performed worse than Protopic,7 and in the 2024 Cochrane analysis, it ranked in the lower tier among non-steroidal topical treatments.5 Tofacitinib 2% ointment also showed only equivalent efficacy when directly compared with pimecrolimus in a phase 3 trial in India (184 participants). In other words, Elidel and tofacitinib are at a similar efficacy level.
So when do we use Elidel? Because it is a cream formulation and clogs pores less, Elidel is a more practical choice for facial atopic dermatitis with acne. Even if it is less effective, treatment only works if you can apply it consistently.
Tofacitinib ointment is not approved in Korea, and long-term data are lacking (only 4-week clinical trials exist), so it is difficult to recommend proactively. In atopic dermatitis communities, some people say, “If you use tofacitinib wrong, you will get an acne explosion,” but this is less about tofacitinib itself and more about the ointment formulation. Because the oils in ointments can clog pores and trigger acne, the same can happen with Protopic as well.
Bepanthen, D-Panthenol | Adjunct

Dexpanthenol 5% (Bepanthen, D-Panthenol) is not an anti-inflammatory medication, but an adjunct that helps repair the skin barrier. There are no studies directly comparing it with Protopic or Elidel, but in pediatric atopic dermatitis trials, it showed efficacy similar to hydrocortisone 1%, the mildest steroid. Because Elidel is also classified in guidelines as comparable to mild steroids, Bepanthen’s anti-inflammatory effect is presumed to be lower than or similar to Elidel. However, because it is an ointment, it can trigger acne, and lanolin—an additive—was selected as the 2023 Contact Allergen of the Year. Since it can cause contact dermatitis in patients with a compromised barrier, it is difficult to recommend as a facial atopic dermatitis ointment.
Hypothetical prescriptions vs. real-world prescriptions
If we ignore regulations and cost and make a hypothetical prescription for facial atopic dermatitis ointments based only on the literature, the order would be as follows. If efficacy is the same, creams are more advantageous than ointments for facial atopic dermatitis, so the first choice would be cream-formulation JAK inhibitors such as Anzupgo, Opzelura, and Rutinib; second, Protopic 0.1%; third, Protopic 0.03%; fourth, Elidel; and fifth, tofacitinib.
But reality is different. In Korea, Anzupgo is approved only for hand eczema, not atopic dermatitis, and the pharmacy acquisition cost is KRW 690,000 for 60 g. Opzelura, Rutinib, and Tofatas are not approved at all, so they can only be obtained via direct purchase. And because Rutinib and Tofatas are drugs approved in Bangladesh and India—where the regulatory environment differs from the U.S. or Korea—it is difficult to know how rigorously they have been validated.
If we limit ourselves to medications approved and covered in Korea, Protopic 0.1% is the most practical first choice if there is no acne, while Elidel is the most practical first choice if there is acne or significant pore blockage. In my own practice, I also prescribe mainly these two, and specifically follow this order:
If the Wood’s lamp exam shows clogged pores or acne → Start with Elidel cream. If the effect is insufficient, switch to Protopic 0.1% ointment.
If the Wood’s lamp exam shows no pore blockage and there is no acne → Start with Protopic 0.1% ointment. If acne develops after use, switch to Elidel cream.
References
- Pariser D. Topical corticosteroids and topical calcineurin inhibitors in the treatment of atopic dermatitis: focus on percutaneous absorption. Am J Ther. 2009;16(3):264-273.
- Hajar T, Leshem YA, Hanifin JM, et al. A systematic review of topical corticosteroid withdrawal (“steroid addiction”) in patients with atopic dermatitis and other dermatoses. J Am Acad Dermatol. 2015;72(3):541-549.e2.
- Coloe J, Zirwas MJ. Allergens in corticosteroid vehicles. Dermatitis. 2008;19(1):38-42.
- Remitz A, De Pità O, Mota A, et al. Position statement: topical calcineurin inhibitors in atopic dermatitis. J Eur Acad Dermatol Venereol. 2018;32(12):2074-2082.
- Lax SJ, Van Vogt E, Candy B, et al. Topical anti-inflammatory treatments for eczema: network meta-analysis. Cochrane Database Syst Rev. 2024;8(8):CD015064.
- Cury Martins J, Martins C, Aoki V, et al. Topical tacrolimus for atopic dermatitis. Cochrane Database Syst Rev. 2015;2015(7):CD009864.
- Paller AS, Lebwohl M, Fleischer AB Jr, et al. Tacrolimus ointment is more effective than pimecrolimus cream with a similar safety profile in the treatment of atopic dermatitis. J Am Acad Dermatol. 2005;52(5):810-822.
- Zhang L, Gong X, Gu Y, et al. Efficacy and safety of treatments for atopic dermatitis: a model-based meta-analysis of randomized controlled trials. Eur J Clin Pharmacol. 2026;82(2):62.
- Chiesa Fuxench ZC, Lai JS, Kuo KL, et al. Ruxolitinib cream monotherapy for facial and/or neck atopic dermatitis: results from a decentralized, randomized phase 2 clinical trial. J Dermatolog Treat. 2025;36(1):2480744.
- Abe M, Igarashi A, Kitajima M, et al. Treatment satisfaction, efficacy, and safety of delgocitinib ointment for atopic dermatitis-induced rash on the face and neck. J Dermatol. 2025;52(8):1232-1242.
Frequently Asked Questions
For facial atopic dermatitis ointments, which is better—ointment or cream?
If you do not have acne, an ointment (Protopic) is advantageous in terms of efficacy and safety. Ointments contain fewer preservatives, so the risk of contact dermatitis is lower. However, if acne develops or worsens after using an ointment, it is more practical to switch to a cream (Elidel).
Is it normal for Protopic to sting and make my skin red?
For the first 2–3 days, TRPV1 receptor stimulation can cause stinging, burning, and redness. It usually settles within a week. Applying it after refrigeration can reduce initial irritation. If it continues to worsen for more than three days, contact dermatitis is possible—stop using it and seek medical care.
Is it okay to use overseas direct-purchase ointments (Opzelura, tofacitinib)?
Products not approved in Korea have not been verified for quality control or bioequivalence. Because Protopic and Elidel can be prescribed in Korea and are covered by insurance, I recommend starting treatment with these medications first.

We treat atopic dermatitis, rosacea, and seborrheic dermatitis.
Thanks to the valuable reviews you have shared in the community, many of you visit us even from far away.
We will repay you with sincere, attentive care.
DK Han
Chief Director, MIRAGEN Clinic
Graduate of University of Michigan, Ross School of Business
Graduate of Chungnam National University School of Medicine
(Former) Representative Director of Ewha Phoenix Rehabilitation Hospital
(Current) Representative Director of MIRAGEN Clinic